
Page 15 - Public Citizen 2021-2022
P. 15
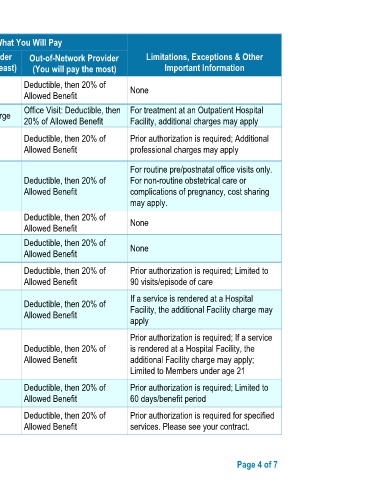
What You Will Pay
Common Services You May Need In-Network Provider Out-of-Network Provider Limitations, Exceptions & Other
Medical Event (You will pay the least) (You will pay the most) Important Information
stay Deductible, then 20% of
Physician/surgeon fee No Charge None
Allowed Benefit
If you have mental Outpatient services Office Visit: No Charge Office Visit: Deductible, then For treatment at an Outpatient Hospital
health, behavioral 20% of Allowed Benefit Facility, additional charges may apply
health, or substance Deductible, then 20% of Prior authorization is required; Additional
abuse services Inpatient services No Charge
Allowed Benefit professional charges may apply
For routine pre/postnatal office visits only.
Deductible, then 20% of For non-routine obstetrical care or
Office visits No Charge
Allowed Benefit complications of pregnancy, cost sharing
may apply.
Childbirth/delivery professional Deductible, then 20% of
If you are pregnant No Charge None
services Allowed Benefit
Childbirth/delivery facility No Charge Deductible, then 20% of None
services Allowed Benefit
Deductible, then 20% of Prior authorization is required; Limited to
Home health care No Charge
Allowed Benefit 90 visits/episode of care
If a service is rendered at a Hospital
Deductible, then 20% of
Rehabilitation services $15 copay per visit Facility, the additional Facility charge may
Allowed Benefit
apply
Prior authorization is required; If a service
Deductible, then 20% of is rendered at a Hospital Facility, the
Habilitation services $15 copay per visit
If you need help Allowed Benefit additional Facility charge may apply;
recovering or have other Limited to Members under age 21
special health needs Deductible, then 20% of Prior authorization is required; Limited to
Skilled nursing care No Charge
Allowed Benefit 60 days/benefit period
Deductible, then 20% of Prior authorization is required for specified
Durable medical equipment No Charge
Allowed Benefit services. Please see your contract.
SBC ID: SBC20210607MANBPPDBL01RXXDB755N072021 Page 4 of 7