
Page 10 - Public Citizen 2021-2022
P. 10
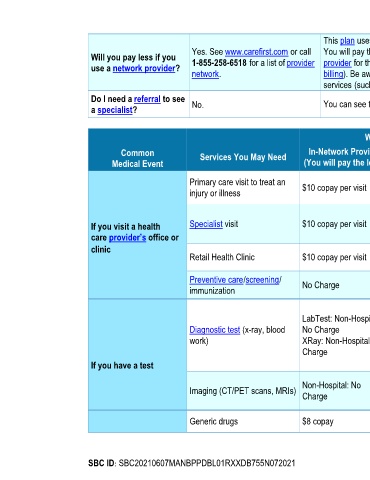
This plan uses a provider network. You will pay less if you use a provider in the plan’s network.
Yes. See www.carefirst.com or call You will pay the most if you use an out-of-network provider, and you might receive a bill from a
Will you pay less if you 1-855-258-6518 for a list of provider provider for the difference between the provider’s charge and what your plan pays (balance
use a network provider?
network. billing). Be aware, your network provider might use an out-of-network provider for some
services (such as lab work). Check with your provider before you get services.
Do I need a referral to see You can see the specialist you choose without a referral.
a specialist? No.
What You Will Pay
Common Services You May Need In-Network Provider Out-of-Network Provider Limitations, Exceptions & Other
Medical Event (You will pay the least) (You will pay the most) Important Information
If a service is rendered at a Hospital
Primary care visit to treat an $10 copay per visit Deductible, then 20% of Facility, the additional Facility charge may
injury or illness Allowed Benefit
apply
If a service is rendered at a Hospital
Deductible, then 20% of
If you visit a health Specialist visit $10 copay per visit Allowed Benefit Facility, the additional Facility charge may
care provider’s office or apply
clinic Deductible, then 20% of
Retail Health Clinic $10 copay per visit None
Allowed Benefit
Preventive care/screening/ No Charge Deductible, then 20% of Some services may have limitations or
immunization Allowed Benefit exclusions based on your contract
LabTest: Non-Hospital:
LabTest: Non-Hospital: Deductible, then 20% of
Diagnostic test (x-ray, blood No Charge Allowed Benefit If a service is rendered at a Hospital
Facility, the additional Facility charge may
work) XRay: Non-Hospital: No XRay: Non-Hospital: apply. Please see your contract.
Charge Deductible, then 20% of
If you have a test Allowed Benefit
If a service is rendered at a Hospital
Non-Hospital: No Non-Hospital: Deductible,
Imaging (CT/PET scans, MRIs) Facility, the additional Facility charge may
Charge then 20% of Allowed Benefit
apply. Please see your contract.
For all prescription drugs:
Generic drugs $8 copay Paid As In-Network
Prior authorization may be required for
SBC ID: SBC20210607MANBPPDBL01RXXDB755N072021 Page 2 of 7