
Page 16 - Public Citizen 2021-2022
P. 16
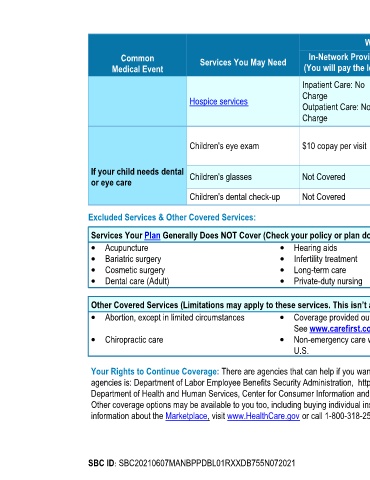
What You Will Pay
Common Services You May Need In-Network Provider Out-of-Network Provider Limitations, Exceptions & Other
Medical Event (You will pay the least) (You will pay the most) Important Information
Inpatient Care: No Inpatient Care: Deductible, Prior authorization is required; Limited to a
Charge then 20% of Allowed Benefit maximum 180 day/benefit period; Inpatient
Hospice services
Outpatient Care: No Outpatient Care: Deductible, Care: Limited to 60 days/Hospice Eligibility
Charge then 20% of Allowed Benefit Period
Member pays expenses in
Children's eye exam $10 copay per visit excess of $33 Allowed Limited to 1 visit/benefit period
Benefit
If your child needs dental Children's glasses Not Covered Not Covered None
or eye care
Children's dental check-up Not Covered Not Covered None
Excluded Services & Other Covered Services:
Services Your Plan Generally Does NOT Cover (Check your policy or plan document for more information and a list of any other excluded services.)
· Acupuncture · Hearing aids · Routine foot care
· Bariatric surgery · Infertility treatment · Weight loss programs
· Cosmetic surgery · Long-term care
· Dental care (Adult) · Private-duty nursing
Other Covered Services (Limitations may apply to these services. This isn’t a complete list. Please see your plan document.)
· Abortion, except in limited circumstances · Coverage provided outside the United States. · Routine eye care (Adult)
See www.carefirst.com
· Chiropractic care · Non-emergency care when traveling outside the
U.S.
Your Rights to Continue Coverage: There are agencies that can help if you want to continue your coverage after it ends. The contact information for those
agencies is: Department of Labor Employee Benefits Security Administration, http://www.dol.gov/ebsa/healthreform, or call 1-866-444-EBSA (3272); or
Department of Health and Human Services, Center for Consumer Information and Insurance Oversight, http://www.cciio.cms.gov, or call 1-877-267-2323 x61565.
Other coverage options may be available to you too, including buying individual insurance coverage through the Health Insurance Marketplace. For more
information about the Marketplace, visit www.HealthCare.gov or call 1-800-318-2596.
SBC ID: SBC20210607MANBPPDBL01RXXDB755N072021 Page 5 of 7