
Page 12 - Public Citizen 2021-2022
P. 12
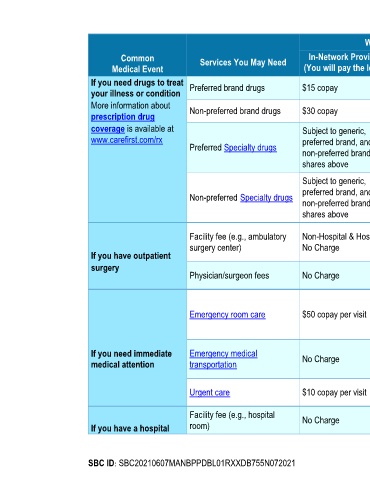
What You Will Pay
Common Services You May Need In-Network Provider Out-of-Network Provider Limitations, Exceptions & Other
Medical Event (You will pay the least) (You will pay the most) Important Information
If you need drugs to treat Preferred brand drugs $15 copay Paid As In-Network certain drugs; No Charge for preventive
your illness or condition drugs or contraceptives; Copay applies to
More information about Non-preferred brand drugs $30 copay Paid As In-Network up to 34-day supply; Up to 90-day supply
prescription drug of maintenance drugs is 2 copays;
coverage is available at Subject to generic,
www.carefirst.com/rx preferred brand, and Specialty Drugs:
Preferred Specialty drugs Not Covered Participating Providers: covered when
non-preferred brand cost purchased through the
shares above
Subject to generic,
preferred brand, and Exclusive Specialty Pharmacy Network
Non-preferred Specialty drugs Not Covered
non-preferred brand cost Non-Participating Providers: Not Covered
shares above
Non-Hospital & Hospital:
Facility fee (e.g., ambulatory Non-Hospital & Hospital:
surgery center) No Charge Deductible, then 20% of None
If you have outpatient Allowed Benefit
surgery Deductible, then 20% of
Physician/surgeon fees No Charge None
Allowed Benefit
Copay waived if admitted; Limited to
Emergency Services or unexpected,
Emergency room care $50 copay per visit Paid As In-Network
urgently required services; Additional
professional charges may apply
Prior authorization is required for air
If you need immediate Emergency medical No Charge Deductible, then 20% of ambulance services, except when
medical attention transportation Allowed Benefit
Medically Necessary in an emergency
Deductible, then 20% of Limited to unexpected, urgently required
Urgent care $10 copay per visit
Allowed Benefit services
Facility fee (e.g., hospital No Charge Deductible, then 20% of Prior authorization is required
If you have a hospital room) Allowed Benefit
SBC ID: SBC20210607MANBPPDBL01RXXDB755N072021 Page 3 of 7