
Page 12 - NAPA 2021-2022
P. 12
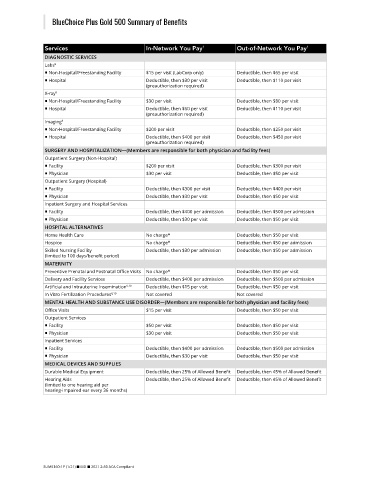
BlueChoice Plus Gold 500 Summary of Benefits
Services In-Network You Pay 1 Out-of-Network You Pay 1
DIAGNOSTIC SERVICES
Labs 9
■ Non-Hospital/Freestanding Facility $15 per visit (LabCorp only) Deductible, then $65 per visit
■ Hospital Deductible, then $30 per visit Deductible, then $110 per visit
(preauthorization required)
X-ray 9
■ Non-Hospital/Freestanding Facility $30 per visit Deductible, then $80 per visit
■ Hospital Deductible, then $60 per visit Deductible, then $110 per visit
(preauthorization required)
Imaging 9
■ Non-Hospital/Freestanding Facility $200 per visit Deductible, then $250 per visit
■ Hospital Deductible, then $400 per visit Deductible, then $450 per visit
(preauthorization required)
SURGERY AND HOSPITALIZATION—(Members are responsible for both physician and facility fees)
Outpatient Surgery (Non-Hospital)
■ Facility $200 per visit Deductible, then $300 per visit
■ Physician $30 per visit Deductible, then $50 per visit
Outpatient Surgery (Hospital)
■ Facility Deductible, then $300 per visit Deductible, then $400 per visit
■ Physician Deductible, then $30 per visit Deductible, then $50 per visit
Inpatient Surgery and Hospital Services
■ Facility Deductible, then $400 per admission Deductible, then $500 per admission
■ Physician Deductible, then $30 per visit Deductible, then $50 per visit
HOSPITAL ALTERNATIVES
Home Health Care No charge* Deductible, then $50 per visit
Hospice No charge* Deductible, then $50 per admission
Skilled Nursing Facility Deductible, then $30 per admission Deductible, then $50 per admission
(limited to 100 days/benefit period)
MATERNITY
Preventive Prenatal and Postnatal Office Visits No charge* Deductible, then $50 per visit
Delivery and Facility Services Deductible, then $400 per admission Deductible, then $500 per admission
Artificial and Intrauterine Insemination 6,10 Deductible, then $15 per visit Deductible, then $50 per visit
In Vitro Fertilization Procedures 6,10 Not covered Not covered
MENTAL HEALTH AND SUBSTANCE USE DISORDER—(Members are responsible for both physician and facility fees)
Office Visits $15 per visit Deductible, then $50 per visit
Outpatient Services
■ Facility $50 per visit Deductible, then $50 per visit
■ Physician $30 per visit Deductible, then $50 per visit
Inpatient Services
■ Facility Deductible, then $400 per admission Deductible, then $500 per admission
■ Physician Deductible, then $30 per visit Deductible, then $50 per visit
MEDICAL DEVICES AND SUPPLIES
Durable Medical Equipment Deductible, then 25% of Allowed Benefit Deductible, then 45% of Allowed Benefit
Hearing Aids Deductible, then 25% of Allowed Benefit Deductible, then 45% of Allowed Benefit
(limited to one hearing aid per
hearing-impaired ear every 36 months)
SUM5160-1P (1/21) ■ MD ■ 2021 2-50 ACA Compliant