
Page 7 - The Legacy School Benefit Booklet 2021-2022
P. 7
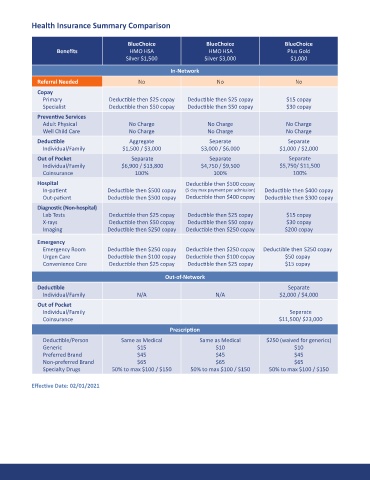
Health Insurance Summary Comparison
BlueChoice BlueChoice BlueChoice
Benefits HMO HSA HMO HSA Plus Gold
Silver $1,500 Silver $3,000 $1,000
In-Network
Referral Needed No No No
Copay
Primary Deductible then $25 copay Deductible then $25 copay $15 copay
Specialist Deductible then $50 copay Deductible then $50 copay $30 copay
Preventive Services
Adult Physical No Charge No Charge No Charge
Well Child Care No Charge No Charge No Charge
Deductible Aggregate Seperate Separate
Individual/Family $1,500 / $3,000 $3,000 / $6,000 $1,000 / $2,000
Out of Pocket Separate Separate Separate
Individual/Family $6,900 / $13,800 $4,750 / $9,500 $5,750/ $11,500
Coinsurance 100% 100% 100%
Hospital Deductible then $500 copay
In-patient Deductible then $500 copay (5 day max payment per admission) Deductible then $400 copay
Out-patient Deductible then $500 copay Deductible then $400 copay Deductible then $300 copay
Diagnostic (Non-hospital)
Lab Tests Deductible then $25 copay Deductible then $25 copay $15 copay
X-rays Deductible then $50 copay Deductible then $50 copay $30 copay
Imaging Deductible then $250 copay Deductible then $250 copay $200 copay
Emergency
Emergency Room Deductible then $250 copay Deductible then $250 copay Deductible then $250 copay
Urgen Care Deductible then $100 copay Deductible then $100 copay $50 copay
Convenience Care Deductible then $25 copay Deductible then $25 copay $15 copay
Out-of-Network
Deductible Separate
Individual/Family N/A N/A $2,000 / $4,000
Out of Pocket
Individual/Family Separate
Coinsurance $11,500/ $23,000
Prescription
Deductible/Person Same as Medical Same as Medical $250 (waived for generics)
Generic $15 $10 $10
Preferred Brand $45 $45 $45
Non-preferred Brand $65 $65 $65
Specialty Drugs 50% to max $100 / $150 50% to max $100 / $150 50% to max $100 / $150
Effective Date: 02/01/2021